Chronic Myeloid Leukemia
On this page
Overview
What is chronic myeloid leukemia (CML)?
Chronic myeloid leukemia (CML), also called chronic myelogenous leukemia, is a cancer of the blood and bone marrow that progresses slowly. CML is linked to the Philadelphia chromosome, a specific genetic abnormality (mutation) found in the bone marrow cells of most patients with CML. It may also show up in patients with acute lymphoblastic leukemia (ALL) or acute myeloid leukemia (AML).
Our approach to chronic myeloid leukemia
UCSF is dedicated to delivering the most advanced treatment options for chronic myeloid leukemia (CML) with care and compassion. For most patients with early-stage CML, medications called tyrosine kinase inhibitors can effectively control the disease for years and will usually prevent it from progressing to the final phase. Should standard treatments fail, UCSF offers stem cell transplants as well as access to clinical trials, which are studies of promising new therapies.
Causes of chronic myeloid leukemia
Genes in your body control cell growth – some promote it, others slow it down. The instructions for this process live in your chromosomes, which are made of inherited DNA. When cells divide, they copy this DNA, and sometimes mutations – changes in the DNA sequence – happen. These differences can impact how your cells grow, which can lead to cancer.
Chronic myeloid leukemia (CML) occurs when something causes genetic changes in myeloid cells – a type of white blood cell – in the bone marrow. It's unclear what triggers this process. But 90% of people with CML have a genetic change, called the Philadelphia chromosome, that leads to immature myeloid cells multiplying out of control.
Risk factors for chronic myeloid leukemia
We don’t know why some people get the gene mutation that causes CML. It's not hereditary. Still, a few risk factors may increase your chances of getting CML, including:
- Sex. CML is slightly more common in men.
- Age. More than half of CML cases develop in people who are 65 or older.
- Extreme radiation exposure. In rare cases, patients who have been exposed to high doses of radiation develop CML. This amount is far beyond the level of radiation you receive from things like dental X-rays and mammograms.
Phases of chronic myeloid leukemia
CML has three main phases. The difference between the phases is based mainly on the number of the immature myeloid cells in the blood or bone marrow and whether they've spread to other parts of the body.
- Chronic phase. CML almost always starts in the chronic phase. At this point, it's usually easy to control with treatment, and patients can lead nearly normal lives.
- Accelerated phase. The disease may progress over a few years into the accelerated phase. If this happens, patients may experience high fever, bone pain and painful enlargement of the spleen.
- Blast phase. This final phase of CML is a form of acute leukemia that's difficult to treat. Tests will show that more than 20% of blood or bone marrow samples are immature white blood cells, known as blasts, and that the blasts have spread to tissues and organs beyond the bone marrow. Patients may experience fever, poor appetite and weight loss.
Symptoms of chronic myeloid leukemia
Most patients with chronic myeloid leukemia (CML) initially visit their doctors because they're experiencing:
- Weakness
- Fatigue
- Shortness of breath
- Low-grade fevers
- Night sweats
- Bone pain
- Weight loss without trying
- Pain or a feeling of abdominal fullness
Many of these symptoms occur because the CML cells are crowding out the bone marrow's healthy red blood cells, white blood cells and platelets.
Diagnosis of chronic myeloid leukemia
Chronic myeloid leukemia (CML) is generally suspected when blood tests show an elevation in white blood cells and there's no illness or infection to account for it.
The diagnosis is confirmed through genetic tests that look for either the Philadelphia chromosome or a gene mutation called BCR-ABL. Either can be responsible for making the myeloid cells grow out of control.
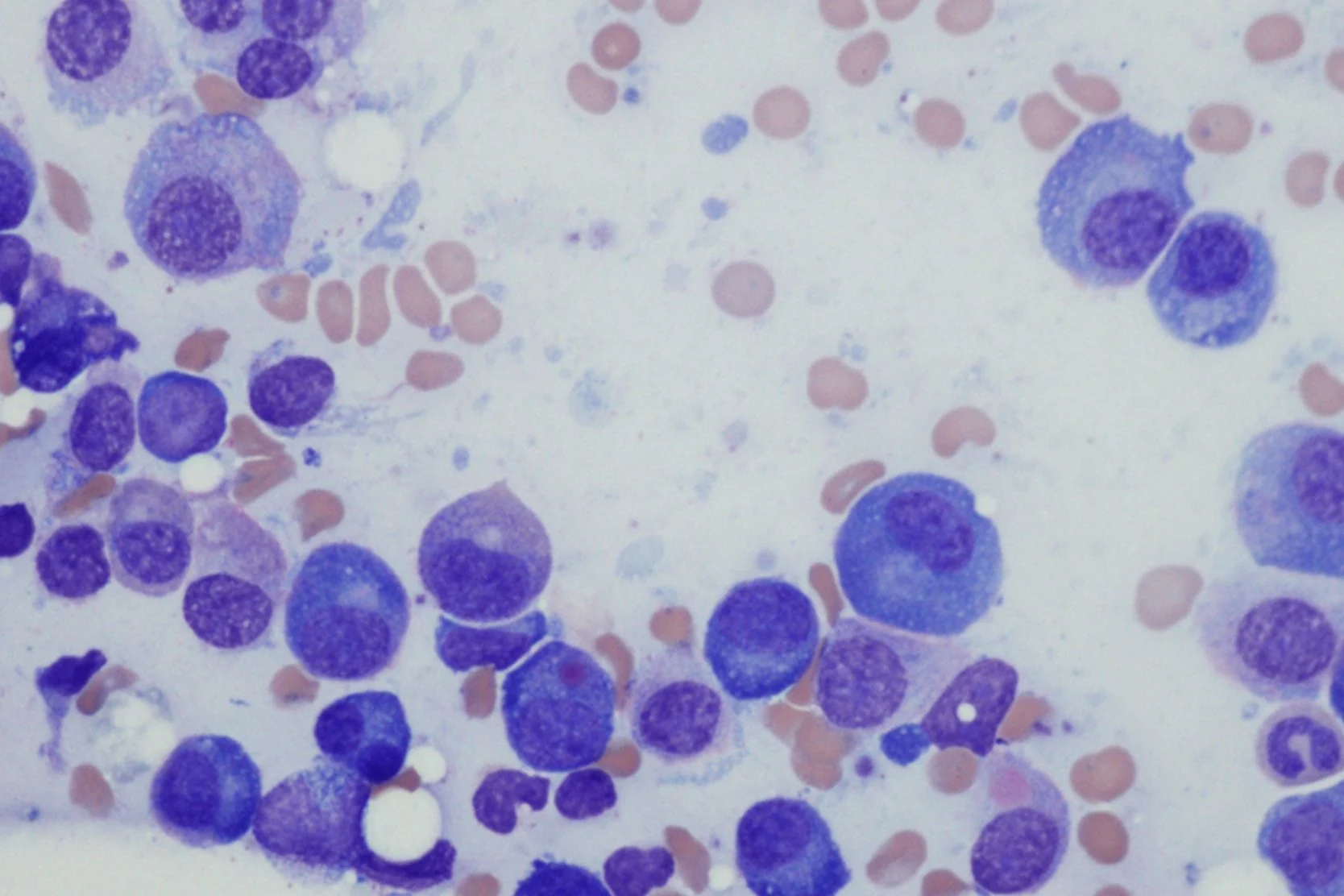
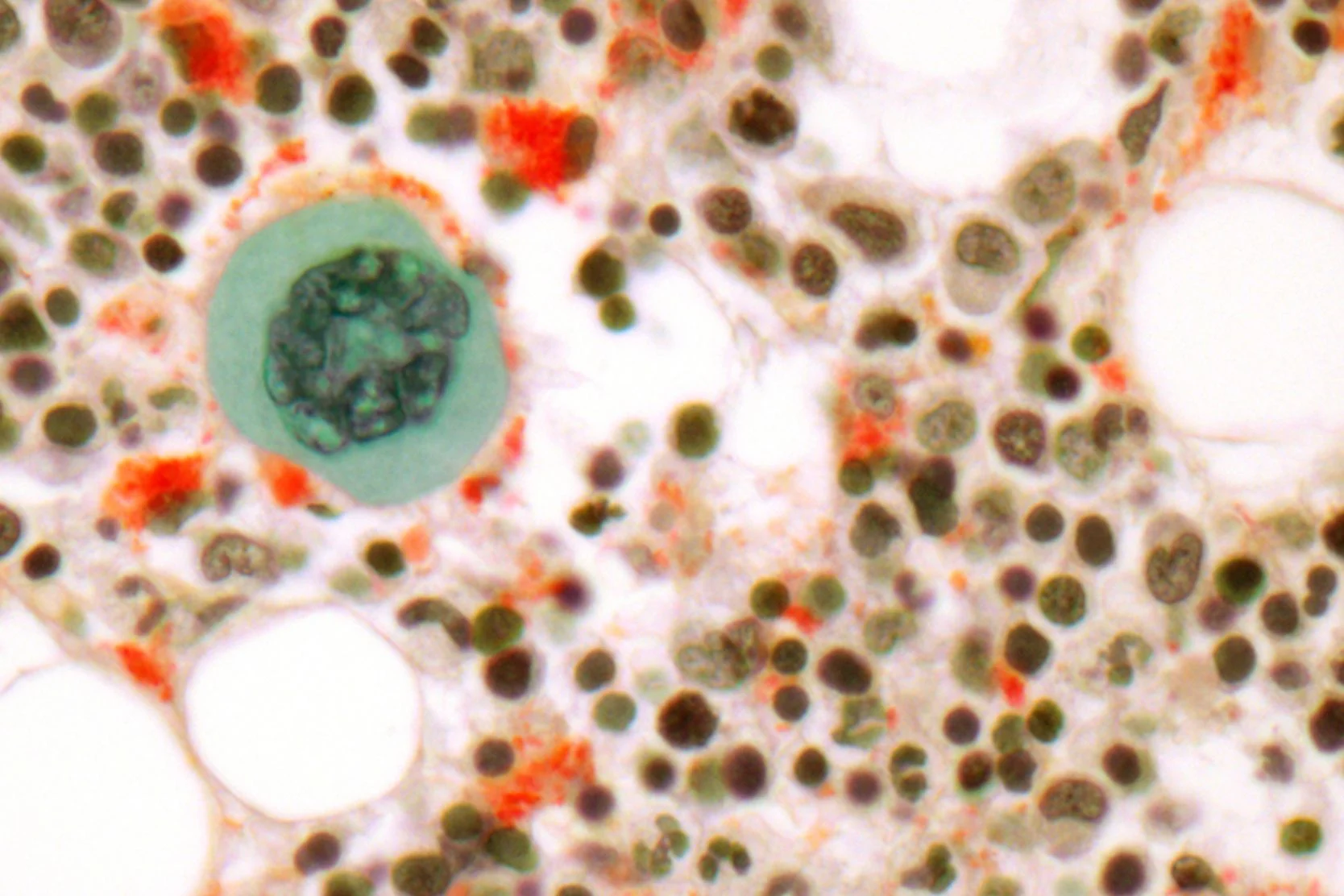
To help determine the stage of the cancer, a bone marrow aspiration (obtaining a sample of fluid) or bone marrow biopsy (obtaining a sample of solid tissue) may be performed so that the leukemia cells can be examined under a microscope.
Treatment of chronic myeloid leukemia
The main treatment for CML is targeted therapy – using drugs or other substances that can identify and attack cancer cells. However, other treatments are available for patients depending on their overall health and the phase of their CML.
Tyrosine kinase inhibitors (TKIs) for CML
Tyrosine kinase inhibitors (TKIs) are drugs used for targeted therapy. They block the protein produced by the BCR-ABL gene that makes white blood cells multiply uncontrollably. These drugs include imatinib (Gleevec), dasatinib (Sprycel) and nilotinib (Tasigna). They're taken orally.
Targeted therapy is effective in 80% of CML patients. In successful cases, the Philadelphia chromosome disappears and normal blood counts are restored. For most patients, TKIs prevent CML from progressing to the accelerated or blast phase.
Patients can survive a long time on TKIs, but whether these drugs actually cure CML is unknown. While taking TKIs, patients are monitored with a blood test every three months and an annual bone marrow aspiration and biopsy.
Stem cell transplantation for CML
Another highly effective option for treating CML is a stem cell or bone marrow transplant (BMT). Typically, the transplant uses stem cells collected from a matched donor, a process called allogeneic transplant. This is a risky procedure, with a treatment-related death rate of 15 to 20%, so it's only for patients who don't respond to TKIs.
Chemotherapy for CML
Chemotherapy used to be a common treatment for CML. However, TKIs are now known to be more effective, so chemotherapy will be used only if TKIs aren't working or as part of a stem cell transplant.
Radiation therapy for CML
Radiation is used only under certain circumstances. For example, it may be used to shrink an enlarged spleen that's causing symptoms, such as loss of appetite. Radiation may also be administered as part of a stem cell transplant or to treat bone pain caused by leukemia cell growth in the bone marrow.
Investigational therapies for CML
UCSF is dedicated to improving outcomes for patients with CML. Interested patients may have opportunities to participate in clinical trials investigating promising treatments for chronic myeloid leukemia.
Awards & recognition

Best in California and No. 7 in the nation for cancer care
Recommended reading
Bone Marrow Transplant Using an Unrelated Donor
Learn about an allogeneic bone marrow transplant, where the bone marrow comes from an unrelated donor. We use HLA typing to find the best match possible.
Hematology and BMT Resource Guide
Learn about hematology conditions and bone marrow transplant (BMT), connect with support groups and find resources that can promote healing and well-being.
Self-Care for Caregivers
Caregiver fatigue can be brought on by the physical and emotional demands of caring for a loved one with a serious illness. Learn tips to combat caregiver fatigue here.
Communicating with Your Doctor
The doctor-patient relationship is built on communication and trust. Get tips to strengthen the partnership between you and your care team.
Coping with Chemotherapy
Everyone experiences chemotherapy differently. Understand the possible emotional and physical side effects of chemotherapy and how to cope.
Delegation to Help with Fatigue
Fatigue caused by cancer treatment can make it hard to accomplish tasks. Learn how to delegate tasks to people you trust and communicate effectively.
Nutrition Plans for Cancer Patients Undergoing Treatment
Side effects of cancer treatment may include a loss of appetite and nausea. Find out what foods to avoid and which ones may help you feel better.
Cancer Pathology Tissue Slides FAQ
If you have a biopsy or surgery, diseased tissue is often placed on slides for a pathologist to examine. Learn how to get the slides to your doctor for review.
Cancer Radiology Scans and Reports FAQ
Learn the difference between a radiology report and radiology films or scans, why your doctor might request the scans and how to get them.
Managing Your Treatment
Living with cancer or caring for someone with the disease can be overwhelming. Here are tips to reduce stress and help navigate life with cancer.
Nutrition and Coping with Cancer Symptoms
Side effects of cancer treatment may affect your eating habits. Find new ways to get the calories, protein and nutrients you need.
Questions to Ask Your Cancer Doctor
These questions can guide conversations with your cancer doctor and help you get the information you need to make care decisions for yourself or a loved one.
Resources for End of Life
Get resources to support yourself and your loved ones through end-of-life issues. Find bereavement support groups, counselors and reading materials.
Tips for Conserving Your Energy
Cancer treatments can cause extreme exhaustion. Here are tips to help you conserve your energy and manage cancer-related fatigue.
Using a Medical Calendar and Symptom Log
Here’s how to keep a medical calendar and symptom log to help you and your doctor track your condition and side effects of treatments or medications.
More treatment info
Allogeneic Transplant
Improvements in supportive care over the past 10 years have improved the results and tolerability of blood and marrow transplants (BMT).Learn more here.
Related services & treatments
Specialties
Conditions
- Leukemia
- Blood Cancer
Treatments
- Targeted Molecular Therapy
- Allogeneic Stem Cell Transplant
- Clinical Trials
Helpful resources
Support services

Art for Recovery
Creativity can help people with serious illnesses cope, heal and express what they're going through. Find out about our program and how to join.
Cancer Exercise Counseling
Our one-on-one exercise training sessions, customized for your needs and abilities, can complement other cancer treatments and speed your recovery.
Cancer Nutrition Counseling
UCSF Health offers free nutrition counseling to our patients with cancer, as well as nutrition seminars that are open to anyone. Learn more.
Cancer Support Groups
These groups offered by the Ida and Joseph Friend Patient and Family Cancer Support Center are free and available to all patients, whether or not you get your health care at UCSF.
Core and More Class for Cancer Patients
A strong body helps you fight cancer and enjoy life. Join this class to stabilize your core, strengthen your muscles and improve overall fitness. For cancer patients and caregivers!
Friend to Friend Specialty Shops
A one-stop boutique for patients with cancer. Get professional help with wigs, prostheses, sun-protective clothing, makeup, skin care and more.
Meditation and Guided Imagery for Cancer Patients
Drop in for a free class designed to help you heal, relax and find balance during your treatment. UCSF and non-UCSF patients are welcome.
Oncology Social Work
Social workers offer support, problem-solving, help accessing UCSF cancer-related resources and more. Find out how to contact the social worker for your clinic.
Patient & Family Cancer Support Center
The center offers wellness programming, community, support groups, classes, workshops and more at no cost to people facing cancer and their loved ones.
Peer Support Programs for Cancer
PeerTalk connects interested cancer patients with cancer survivors who can share their own experience to provide emotional and practical support.
UCSF Health medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your provider.