Transcatheter Aortic Valve Replacement (TAVR)
On this page
What is transcatheter aortic valve replacement (TAVR)?
Transcatheter aortic valve replacement (TAVR), sometimes called transcatheter aortic valve implantation (TAVI), is a minimally invasive procedure for treating aortic valve stenosis. As blood exits the heart, it passes through the aortic valve. In patients with aortic stenosis, the valve is stiff and narrow and doesn't open and close properly. This makes it harder for the heart to pump blood to the body.
As a result, patients feel short of breath and fatigued, and are at high risk for a heart attack.
The only treatment for aortic valve stenosis is to replace the faulty valve, which traditionally required open-heart surgery. For many patients, however, there is an equally effective, much less invasive alternative – TAVR.
How is the TAVR procedure done?
Instead of opening the chest to remove and replace the damaged valve, the doctor threads a catheter, a thin, flexible tube, through a blood vessel to reach the heart. The catheter is usually threaded through the groin or the chest. Then, the doctor inserts a new valve using the catheter, positioning it inside of the faulty valve to restore healthy blood flow. The TAVR procedure takes much less time than open-heart surgery, and patients recover more quickly, with less pain and scarring.
UCSF has a comprehensive valve program that offers catheter-based treatment options for all four valves in the heart.
Evaluation for TAVR
Initially, TAVR was intended for patients who were at too high a risk to undergo open-heart surgery. Now, it is approved for anyone with severe aortic stenosis. To determine whether it's a good option for you, our team of heart specialists will evaluate your heart health as well as your overall health. You may have all or some of the following tests as part of the evaluation:
- Blood tests. These tests help doctors assess your health. They will likely include a red blood cell count, which indicates how much oxygen is being delivered to your body's cells; electrolyte levels, which can be disturbed by an underlying illness; and tests to measure substances in the bloodstream that reflect how well your kidneys, liver and thyroid are working.
- Chest X-ray. This exam can show the size of your heart and reveal whether you have fluid buildup in your lungs.
- Electrocardiogram (EKG). This is a painless test to assess the heart's electrical activity. Electrodes are taped to your chest, arms and legs to record and measure the signals that cause your heart to beat.
- Transesophageal echocardiogram (TEE). During a TEE, an ultrasound probe is inserted into your esophagus to capture clear images of your heart's chambers and valves. These images are used to assess how blood flows through your heart.
- Cardiac MRI or CT scan. These exams provide detailed images of your blood vessels, the blood flow through your heart, and your heart's structure and motion.
- Right heart catheterization. This exam may be performed to collect more information about how well your heart is pumping. A catheter is inserted through a blood vessel and threaded into the heart, where it measures the blood pressure in your heart and in the main arteries of your lungs. The catheter can also measure cardiac output and blood oxygen levels.
If your doctor suspects that you have coronary artery disease (CAD) in addition to aortic stenosis, you may also have these tests:
- Coronary angiogram. This provides images of the heart's blood vessels to detect blockages. During this test, a catheter is inserted into a blood vessel (usually in the groin area) and threaded up to the heart. A contrast dye (a harmless substance that shows up well on X-rays) is injected through the catheter, and X-ray images track the blood flow to your heart muscle.
- Exercise stress test. This shows your heart's response to exertion. You'll either be given medication that makes your heart work extra hard, or asked to exercise (on a treadmill or stationary bike), while we track your vital signs and monitor your heart's response.
If your tests indicate that you would benefit from TAVR, our cardiac care team will develop a treatment plan for you. Each patient's team includes a cardiologist, cardiac surgeon, interventional cardiologist, nurse practitioner and imaging specialist.
Preparing for a TAVR
Our team will set you up for an appointment with the UCSF Prepare Program. The program staff are dedicated to preparing you for your scheduled procedure, including ensuring you complete all required testing. They will review your medications to be certain you have the correct instructions regarding their use and will discuss your pain control options. They will share all their communication and information with the TAVR team.
How you can prepare for your TAVR procedure:
- Talk to your doctor about your medications. Find out which ones you should or shouldn't take on the days leading up to your procedure, on the day itself, and on the following days.
- Get a dental checkup. Oral bacteria can infect the heart valve.
- Make a recovery plan. It's important to work out details, such as who will take you home, stay with you at home, and do things like help you prepare meals.
TAVR Procedure
We perform TAVR procedures in a state-of-the-art operating room at the UCSF Helen Diller Medical Center at Parnassus Heights. Before the procedure, you will have an echocardiogram, then we will bring you to the operating room.
Our team will have already determined the type of anesthesia they'll use for you, as the best choice depends on certain health factors. You may be given general anesthesia where you are fully asleep, or a sedative that leaves you awake but relaxed and not feeling pain.
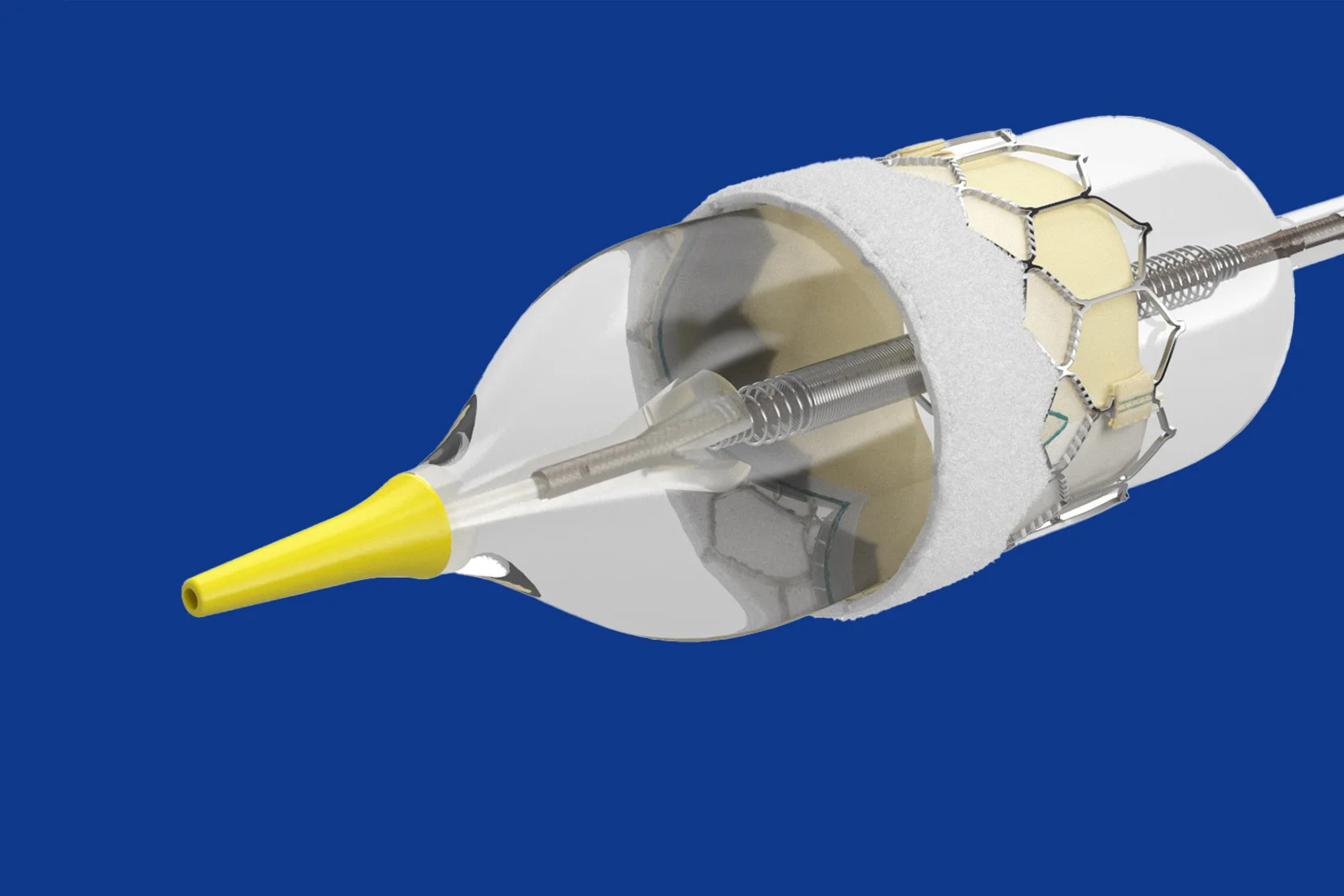
Once you are under anesthesia, the doctor will make a small incision in either your groin or chest and insert a catheter into the major artery there. The doctor will use this to convey a new valve to your heart. The new valve is collapsed so it can pass easily through the catheter to your heart.
As part of the procedure, we will place a temporary pacemaker to ensure your heartbeat stays regular. In many patients, we also place a filtration device inside a blood vessel in your neck. This device lowers the risk of stroke by capturing any tiny bits of plaque that come loose during the procedure, preventing them from reaching the brain. The device is inserted through a small incision in your wrist.
Once the replacement valve is inside your damaged valve, the new valve is expanded to full size. It then pushes aside the "leaflets" of the old valve – the flaps that open and close – and takes over the job of regulating blood flow from the heart. The new valve is typically made of bovine (cow) or porcine (pig) tissue; both are compatible with human tissue.
After we place the valve, we remove the temporary pacemaker. If we detect a slow heart rate, however, we may wait until the following day to remove it. The filtration device in your neck is also removed. The whole operation takes about two to three hours – half as long as open-heart surgery.
Another echocardiogram is performed immediately after the procedure to assess how the new valve is functioning. Once that's completed, you'll be taken to the recovery area.
Recovery from TAVR
Immediately after the procedure, you'll recover in the post-anesthesia care unit. You'll then be transferred to either our transitional care or intensive care unit, depending on the level of care you need.
Patients are encouraged to be up and walking within 24 hours. Most patients spend one to two nights in the hospital, where they are closely monitored. During your hospital stay, your cardiac care team will conduct several follow-up tests, including a chest X-ray, EKG and echocardiogram, to ensure your heart is functioning properly.
Before you go home, your team will talk with you about caring for yourself. They’ll cover topics such as diet, exercise, care of your incision sites, and any new medications.
After discharge, you'll need to have regular checkups with your primary care doctor, local cardiologist and the heart team, as necessary. These checkups are important to ensure all is well with your new valve and to detect any potential problems early.
Particularly during the first weeks of recovery at home, you'll need to be mindful of how you're feeling. If you experience unusual headaches, dizziness or other concerning symptoms, immediately call the doctor who performed your procedure or dial 911.
We advise patients not to drive for at least 72 hours after the procedure (to allow the incisions to heal) and to avoid strenuous physical activity for 10 days. TAVR recovery is much faster than recovery from open-heart surgery, and most patients can resume normal activities within two weeks. However, it may take one to two months for a full recovery.
You can talk to one of our social workers about the help and care you may need at home as you heal. Some patients may require a homecare nurse or a cardiac rehabilitation program after a TAVR.
This program includes a team of health care professionals who provide an individualized exercise plan, education and support to help you improve your heart health and quality of life. Ask your doctor whether cardiac rehab is right for you.
Awards & recognition

One of the nation's best for heart & vascular care

Rated high-performing hospital for aortic valve surgery
Rated high-performing hospital for transcatheter aortic valve replacement
Related services & conditions
Specialties
Conditions
- Aortic Valve Disease
UCSF Health medical specialists have reviewed this information. It is for educational purposes only and is not intended to replace the advice of your doctor or other health care provider. We encourage you to discuss any questions or concerns you may have with your provider.